Thyroid Gland
Category : 11th Class
The name "thyroid" was introduced by Thomas Wharton (1656). It is derived from Greek "Thyreos" a shield.
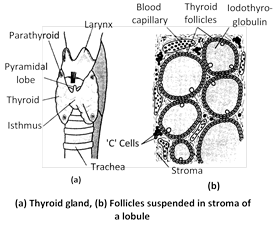
Location : This is the largest endocrine gland of our body. It is located in our neck upon the ventral aspect of larynx (sound box or Adam's apple) and a few anteriomost tracheal rings. It is a dark brown and H-shaped/butterfly bilobed gland.
Origin : It is endodermal in origin and arises in the embryo as a midventral process from the floor of the tongue in pharyngeal region between the first and second pharyngeal pouches. Later, the duct-like connection (thyroglossal duct) of the process degenerates, so that the process is separated from the tongue and becomes endocrine. Probably, the gland is homologous to the endostyle of lower chordates.
Structure of thyroid gland : In adult human beings, thyroid gland measures about 5 cm in length and 3 cm in width. It's average weight is 30 grams. It is somewhat larger in women. In old age, it becomes somewhat smaller as age advances. Its two lobes are connected by a narrower isthmus formed of nonglandular connective tissue. A small, conical pyramidal lobe is often found extended forwards from the isthmus. The whole gland is enveloped by a fibrous capsule. Thin septa or trabeculae, extending inwards from the capsule, divide the gland into a number of lobules. Each lobule, in turn, consists of a large number of small and hollow, spherical follicles (acini) embedded in a small amount of a loose connective tissue that forms the stroma of the gland.
The wall of each thyroid consists of a single-layered cuboidal epithelium suspended from a basal lamina, while its cavity is filled with a yellowish, jelly-like and iodinated colloid glycoprotein substance, called iodothyroglobulin. Besides containing a dense network of blood capillaries, the stroma contains small clusters of specialized parafollicular or 'C' cells. The latter are remnants of ultimobranchial bodies derived from the fifth pharyngeal (branchial) pouches in the embryo.
Synthesis and storage of iodothyroglobulin : Synthesis of a glycoprotein thyroglobulin (TGB) - occurs continuosly in the follicular cells under genic control. The cells keep extruding thyroglobulin in follicular cavity by exocytosis. Each molecule of thyroglobulin contains about 500 amino acid momoners of which 123 monomers are of tyrosine at fixed places. Soon as the molecules of iodine and thyroglobulin come out of follicular cells, these interact in such a way that 15 tyrosine monomers of each thyroglubulin molecule at fixed places become iodinated. Certain tyrosine monomers bind with single atoms of iodine, forming monoiodotyrosine (MIT or \[{{T}_{1}}\]). Other tyrosine monomers bind with two atoms of iodine, forming diiodotyrosine (DIT or \[{{T}_{2}}\]). This is called organification of thyroglobulin. Molecules of iodothyroglobulin keep accumulating in follicular cavity, forming the jelly-like colloid. Within the colloid, molecules of iodothyroglobulin undergo conformational changes and may even interact with each other. This results in a coupling of most of the iodinated tyrosine monomers in pairs. This coupling may occur between the iodinated tyrosine monomers of the same or different molecules of iodothyroglobulin. It results in the formation of several groups of complexes of tetraiodothyronine (thyroxine – T4) and some of triiodothyronine (T3) in the colloid. Each T4 complex obviously contains two tyrosine monomers and four atoms of iodine, whereas each triiodothyronine complex contain two tyrosine monomers and three atoms of iodine. \[{{T}_{4}}\] and \[{{T}_{3}}\] are actually the iodinated hormones secreted by thyroid. Obviously, the colloid acts as a reservoir of these hormones.
The daily output of thyroid glands is about \[80\,\mu g\,\,(0.08\,\,mg)\] of \[{{T}_{4}}\] and about 4mg of \[{{T}_{3}}.\] Since, however \[{{T}_{3}}\]is several times more potent, most of the \[{{T}_{4}}\] molecules also change into T3 molecules by losing one iodine atom as these diffuse from blood into ECF. This deiodination of \[{{T}_{4}}\] is maximum in the liver.
As described in a preceding account, the rate of thyroid secretion is controlled by pituitary gland and the hypothalamus of brain respectively under direct and indirect negative feedback regulation. Rate of thyroid secretion increases during winters and in pregnant women.
Synthesis and secretion of iodinated hormones
Iodides and Iodine : An adult human body contains about 5 to 6 milligram of iodine and most of it is found in thyroid gland. Thus, the thyroid is a reservoir or iodine. For secreting the iodinated hormones in normal amounts, the thyroid daily utilizes about 150 micrograms (0.15 milligram) of iodine. Obviously, a person must daily obtain \[150\,\,\mu g\] of iodine from food. We can obtain this from dairy products, drinking water, seafood, etc. If obtained more than this, we excrete the excess iodine in urine.
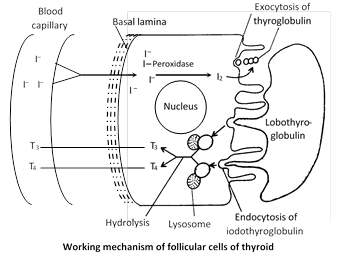
Iodine of food is absorbed and circulated in blood in the form of iodide ions \[({{I}^{}}).\] Follicular cells of thyroid very actively obtain these ions from blood by active transport. That is why, the concentration of \[{{I}^{}}\] in these cells normally remains about 50 to 250 times more than in blood. These cells possess peroxidase enzyme in abundance. Peroxidase continuosly oxidizes iodide ions into molecular iodine (2I–®I2). Iodine is, then, released by follicular cells into follicular cavity.
Hormones of thyroid
Thyroid gland secretes two iodinated hormones. Thyroxine \[({{T}_{4}})\] and Tri iodothyronine \[({{T}_{3}})\] and one non iodinated hormone thyrocalcitonin. Secretion of thyroid gland is regulated by TSH of anterior pituitary lobe. Thyroxine was first isolated by Kocher (1914) but was first crystalized by Kendall (1919). Its molecular structure was given by Harrington and Berger (1927). They also synthesized thyroxine.
(1) Thyroxine : It is an iodine containing (6% iodine) amine hormone which is derived from tyrosine amino acid. Chemically thyroxine is tetraidothyronine though also found as tri-iodothyronine. Secretion of thyroxine is inversely proportional to the blood level of thyroxine (feed back mechanism). These hormones perform following functions :
(i) These regulate Basal Metabolic Rate (BMR) of the body as control rate of cell respiration and energy production in mitochondria hence the "Tempo. of life". So these control physical, mental and sexual growth of body. It is called calorigenic effect.
(ii) In 1912 Gudernatsch discovered that metamorphosis in frog's tadpole begins only when adequate amount of thyroxine is secreted by the thyroid of the tadpole. It was also found that hyposecretion of thyroxine retards and hypersecretion enhances the rate of metamorphosis.
In the hilly tracts of North America from whose soil all iodine has been washed away by rain water, the tadpoles of Ambystoma probably never metamorphose. Therefore, these tadpoles grow to a large size and attain sexual maturity, i.e., these become paedogenetic larvae. This phenomenon is called paedogenesis. The paedogenetic larvae of Ambystoma are called Axolotl larvae.
Addition of thyroxine or iodine in pond water naturally induces and enhances metamorphosis in the tadpoles.
(iii) Functions of osmo-regulation and regulation of moulting have been ascribed to these thyroid hormones in cold-blooded vertebrates (fishes, amphibians and reptiles).
(iv) These control working by renal tubules of kidney so control urine output.
(v) These help in homeothermy in warm blooded animals.
(vi) Synthesis of additional sodiumpotassium pump (\[N{{a}^{+}}/{{K}^{+}}\]ATPase), which then use more ATP more heat is given off, and body temperature rises. This phenomenon is called calorigenic effect of thyroid hormone, and thus maintain normal body temperature.
(2) Thyrocalcitonin (TCT) : It is a long peptide hormone secreted by parafollicular cells of thyroid gland (C-cells). It's secretion is regulated by increased plasma level of calcium by feedback mechanism. TCT lower calcium level in blood to normal by -
Increasing calcium deposition in the bones, so checks osteoporosis and stimulates excretion of calcium in urine. Its prevent hypercalcaemia. Decreasing reabsorption of calcium from urine, so increasing excretion of \[C{{a}^{2+}}.\] So it prevent hypercalcaemia.
Irregularities of thyroid gland
(1) Hypothyroidism : (Decreased secretion of thyroxine from thyroid gland). It leads to the following diseases -
(i) Cretinism : It is disease of infants, called cretins. It is characterised by Decreased BMR (50% than normal); stunted growth; retarded mental development so low I.Q., delayed puberty; decreased body temperature, heart rate, pulse rate, blood pressure and cardiac output; reduced urine output; decreased sugar level in blood, pigeon's chest (chest bulging forward in sternal region). Cretinism can be congenital (absence of thyroid due to genetic defect) or endemic (absence of iodine in diet). It can be corrected by thyroxin administration.
(ii) Myxoedema : It occurs due to deficiency of thyroxine in adults like cretinism, it also has low (BMR) (by\[3040\,%\]); low body temperature, reduced heart rate, pulse rate, blood pressure and cardiac output, low sugar and iodine level in blood etc. But the peculiar feature of myxoedema is that face and hands become swollen due to deposition of albuminous myxomatous tissue. It can also be corrected by thyroxine administration.
(iii) Endemic or simple goitre or colloid goitre : It occurs due to deficiency of iodine in drinking water. It is non-genetic (sporadic goitre is a genetic disease). It is characterized by enlargement of thyroid gland due to increase in number and size of acinal cells of thyroid gland. It is more common in people of hilly region. To prevent goitre, the table salt is being iodised these days.
(iv) Hashimoto's disease : It is called auto-immune thyroiditis and occurs due to age factor, injury-surgery, wrong treatment or injection thyroid gland causing hyposecretion of thyroxine. When thyroxine secretion falls upto minimal limit, the antibodies are formed which destroy the thyroid gland.
(2) Hypersecretion of thyroid hormones (Hyperthyroidism or thyrotoxicosis) : This may also be a genetic defect, but usually it is provided by chronic infections (influenza, rheumatism, tonsilitis, tuberculosis, measles, whooping cough, etc.) pregnancy, intake of large doses of iodine, over-eating, etc. It results into a considerable increase in glucose and oxygen consumption by cells and the rate of oxidative metabolism in the mitochondria. Consequently, the BMR (basal metabolic rate) may increase severalfolds (hypermetabolism). The cells fail to store all catabolic energy into ATP. Consequently, the extra energy is liberated as heat. Instead of causing growth of body, this energy, thus, overheats the body, causing nervous tension and excitement, restlessness and anxiety, muscular weakness (thyrotoxic myopathy), fatigue and tremors, high temperature, palpitation of heart, copious sweating, diarrhoea, insomnia, trembling of limbs and body, weight loss, heat intolerance, warm and soft skin, increased appetite, etc.
Under his "Sodium pump theory of thermogenesis". Edelman has recently (1974) hypothesized that overheating of body in hyperthyroidism is not because cells fail to trap the excess catabolic energy in ATP, but because the excess ATP formed in this condition is utilized in considerably accelerating the \[N{{a}^{+}}{{K}^{+}}\] pump, relesing more heat that overheats the body.
(i) Simple goitre : Hyperthyroidism may be simply because of overactive cells of a normal gland, or because of an enlargement of the gland, causing goitre.
(ii) Exophthalmic goitre : Such a goitre is called exophthalmic goitre, because it is usually accompanied with some asymmetrical protrusion (Exophthalmos) of the eyeballs, imparting an angry, frightened, or staring look to the patient. Protrusion of eyeballs is due to accumulation of mucus in eye orbits.
(iii) Grave’s or Basedow's disease : Enlargement of the gland is usually due to a diffused growth.
(iv) Plummer's disease or Toxic Adenoma : It is due to formation of one or more hypersecretoy nodules plummer's diseases or Toxic Adenoma in the gland.




You need to login to perform this action.
You will be redirected in
3 sec

